Long-Term Biologic Costs: Do You Need to Shave Teeth for Veneers?
In the context of long-term prognosis and treatment planning, the question do you need to shave teeth for veneers must be weighed against the biological cost of the procedure over the patient's lifetime. As a senior consultant at The Gentle Care Hub, I evaluate dental interventions not just by their immediate aesthetic impact, but by their failure rates and biological consequences at the 10, 15, and 20-year marks. The decision to reduce tooth structure is a decision to enter the "Restorative Cycle," a lifelong commitment to maintaining and replacing artificial materials.
The Spectrum of Invasiveness
We must view the preparation of teeth on a spectrum.
Enamel Preservation is Key
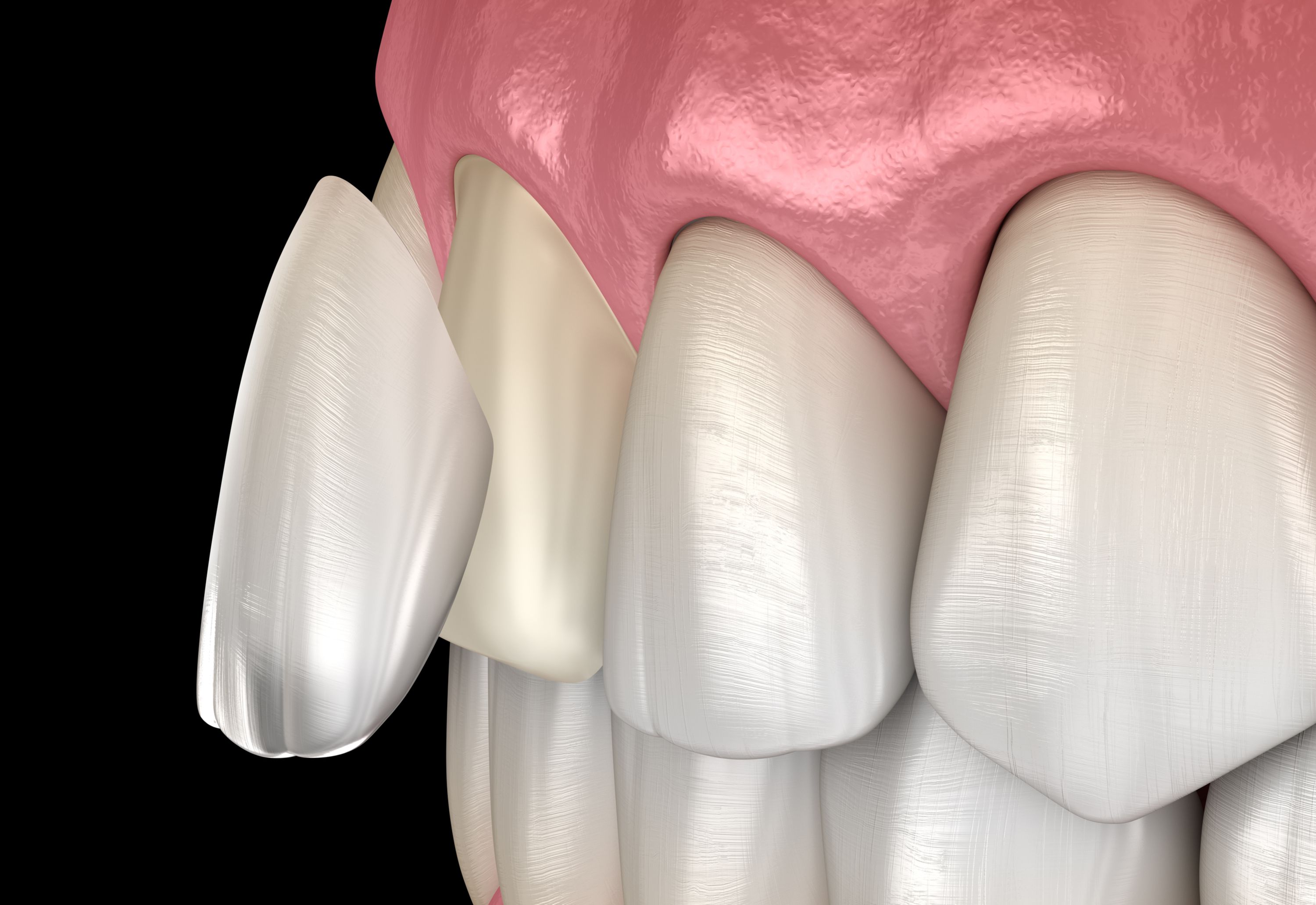
The long-term survival of a veneer is strictly dependent on bonding to enamel. Bond strengths to dentin are significantly weaker and degrade over time due to hydrolysis. When evaluating do you need to shave teeth for veneers, the "safe zone" is strictly within the enamel layer. Aggressive reduction that exposes dentin increases the risk of debonding and flexural failure. However, "zero reduction" (no-prep) sits at the other end of the risk spectrum. While it preserves enamel, it often compromises periodontal health due to poor contours. The ideal prognostic sweet spot is "minimal preparation" (0.3mm-0.5mm), which balances bond strength with periodontal integrity.
The Cost of Reversibility
A common misconception driving the "no-prep" trend is the desire for reversibility.
The Fallacy of "Going Back"
Patients ask do you need to shave teeth for veneers hoping that if they say "no," they can pop the veneers off later and return to their natural smile. In reality, even no-prep veneers require etching the enamel surface with phosphoric acid and bonding with resin. Removing these veneers requires rotary instrumentation (drilling) to grind away the ceramic and resin. It is virtually impossible to remove a bonded veneer without scratching or altering the underlying enamel. Therefore, from a risk management perspective, I advise patients to view all veneer procedures as irreversible events. The decision should not be based on "can I go back?" but "am I willing to maintain this forward?"
Endodontic Risks and Pulpal Health
Whenever a tooth is cut, the pulp (nerve) is insulted.
The Cumulative Trauma
With aggressive preparation (crown-style preps for veneers), approximately 1-5% of teeth may eventually require root canal therapy due to pulpal necrosis. By keeping the preparation minimal—just enough to satisfy the material thickness—we minimize thermal trauma to the pulp. When answering do you need to shave teeth for veneers, we must ensure the reduction depth does not violate the proximity to the pulp horns. Minimal prep veneers have a statistically negligible risk of endodontic complications compared to aggressive full-coverage preparations.
Prognosis of No-Prep vs. Prep
Longitudinal studies indicate distinct failure modes for both approaches.
Periodontal Failure vs. Mechanical Failure
No-prep veneers often fail "biologically"—meaning the gums recede or become infected due to the bulky margins, necessitating removal. Prepped veneers, if done aggressively, fail "mechanically" (debonding from dentin). The highest success rates are found in cases where the dentist performs strategic, minimal reduction confined to the enamel. This approach respects the biology of the gums while ensuring the mechanics of the bond.

Ultimately, to answer the question, "Do my teeth need to be shaved in order to get veneers?" and ensure a successful long-term outcome, the data suggests that strategic, minimal reduction offers the best prognosis. It avoids the periodontal pitfalls of bulky no-prep veneers while avoiding the structural risks of aggressive preparation. It is a calculated biological cost paid upfront to ensure decades of stability and health.
